Holistic Healing- Combining Physiotherapy With Yoga & Pilates.
2025-08-23T11:04:07  read more
read more
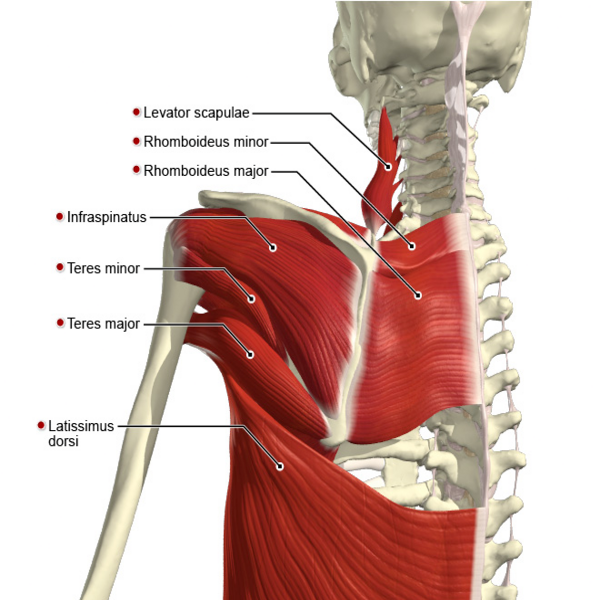

Scapular Dyskinesia Scapular dyskinesia refers to abnormal movement or positioning of the scapula. While often confused with scapular winging, the two are distinct—scapular winging typically results from long thoracic or spinal accessory nerve injury and can lead to SD. SD is common in overhead athletes and individuals with shoulder issues such as rotator cuff injuries, impingement, instability, or labral tears. It can also occur in asymptomatic individuals. Subacromial impingement often presents with reduced scapular upward rotation, external rotation, and posterior tilt. Although SD is linked with shoulder pain, it remains unclear whether it is a cause or effect. Some studies suggest SD may predict future shoulder pain. Scapular movement includes: Motions: Upward/Downward Rotation Internal/External Rotation Anterior/Posterior Tilt Translations: Vertical (up/down) gliding on the thorax Medial/Lateral gliding around the ribcage Clinical Presentation SD can be symptomatic or not. Symptoms may include: Anterior, superior, or posterosuperior scapular pain Neck pain Shoulder impingement or instability Rotator cuff dysfunction Proximal lateral arm pain Thoracic outlet-like symptoms Physiotherapy Management of Scapular Dyskinesia- Treatment focuses on restoring scapular retraction, posterior tilt, and external rotation. Key interventions include: Flexibility Exercises: Stretching the pectoralis minor Shoulder horizontal abduction at 90° and 150° elevation Stabilization & Strengthening: Open/closed-chain exercises: push-ups, lawnmower exercises, resisted retractions Serratus anterior and trapezius strengthening (essential for scapular stability and overhead function) Push-ups on stable surfaces (target serratus anterior); unstable surfaces (increase trapezius activation) Shrug exercises (engage upper/lower trapezius and promote upward rotation) – avoid during early rehab (first 4–6 weeks) to prevent imbalance

We hate spam too.
